
Genetics of NBIA
Here, we've compiled basics on genetic issues related to NBIA.
The information provided here can only provide rough guidance and does not cover every individual case, which is why we strongly recommend that all affected families seek genetic counseling. Please contact the genetics laboratory that made the NBIA diagnosis. The costs are usually covered by health insurance.
NBIA is genetically very diverse. More than 15 genes have been described in the literature so far (see What is NBIA?). Other genetic causes are currently being researched. NBIA diseases that cannot (yet) be assigned to any of the known genes are called idiopathic NBIA.
Human genes are normally located on 46 chromosomes, 23 each from the mother and the father. 22 of these chromosome pairs are called autosomes, 1 pair of chromosomes is called sex chromosomes (gonosomes, X/Y). Women usually carry two functioning copies of all genes. Since men have only one X chromosome in the sex chromosomes, they lack a backup copy for the genes encoded there. The karyogram on the right shows all 23 pairs of chromosomes in a man.
If a person carries a mutated, i.e. defective, copy of a gene, he or she is a carrier of the mutation. In the case of recessive genes, a mutation in one of the two copies has no consequences for the carrier and the disease only breaks out if both copies of the gene would have a mutation. This is referred to as autosomal recessive inheritance. This is how most NBIA diseases are inherited.
Only a few NBIA diseases are inherited in an autosomal dominant manner, i.e. a mutated copy of the gene is sufficient to cause the disease to break out.
Another exception is BPAN. In this case, the mutation almost always arises spontaneously in the child, usually shortly after fertilization or already in the germline. This is referred to as a new mutation or de novo mutation.
Inheritance of most NBIA disorders
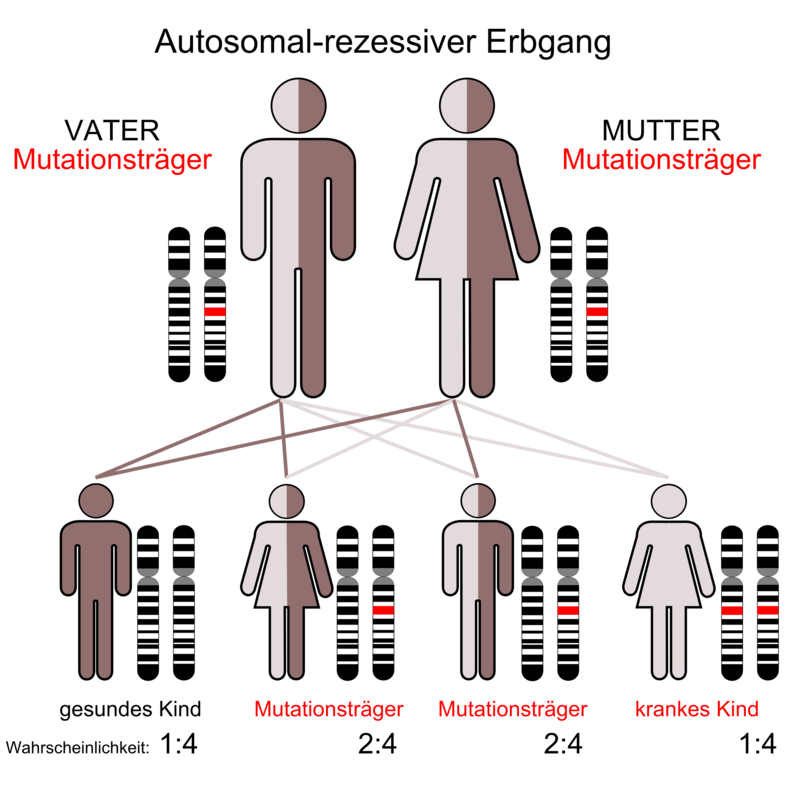
If one copy of a recessive gene carries a change (mutation), the "carrier" of the mutation is healthy, but can inherit the mutated gene. Recessive disorders only occur when both parents are carriers of the same condition and both pass on the mutated gene to their child. Statistically, the probability is 1 in 4 (25%) that two carriers will have a child affected by NBIA, 2 in 4 (50%) of having a child who is also a carrier, and 1 in 4 (25%) of having a child to whom the gene mutation has not been passed on. Most NBIA diseases are inherited in this way, i.e. autosomal recessive.
Exceptions
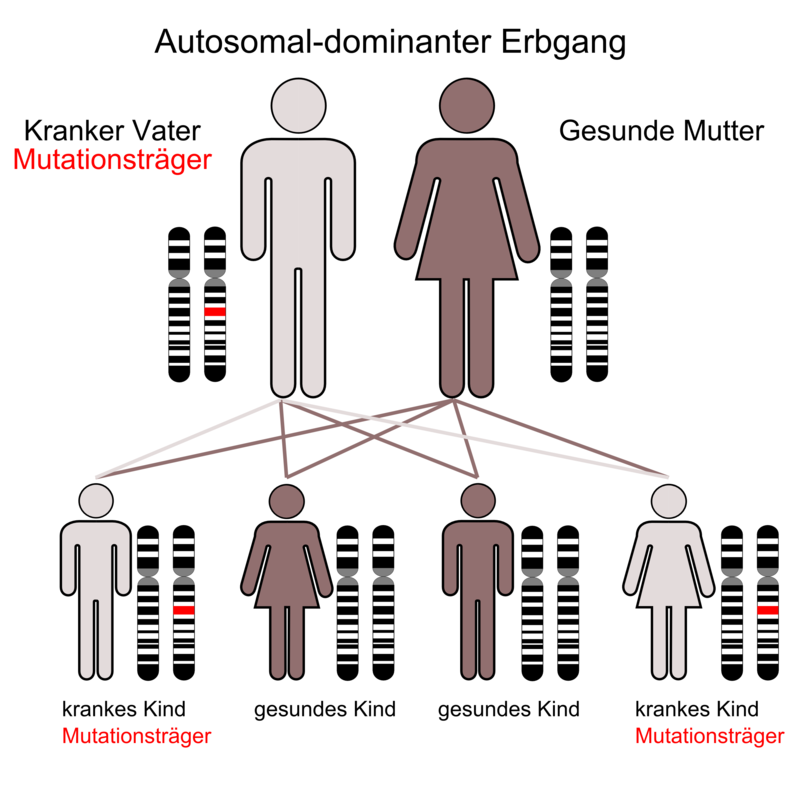
In autosomal dominant inheritance, a mutated copy of the gene from a parent who is usually affected is sufficient to cause the disease in the children as well. The probability that an affected person will pass on the altered gene to one of their children is 1 in 2 (50%).
As far as is known, this inheritance only plays a role in two NBIA diseases: Neuroferritinopathy is always inherited in an autosomal dominant manner and is MPAN, which is usually inherited in an autosomal recessive manner, this inheritance has also been proven in some cases. You can also read the article: "MPAN can also be inherited in an autosomal dominant manner"
New mutation in BPAN
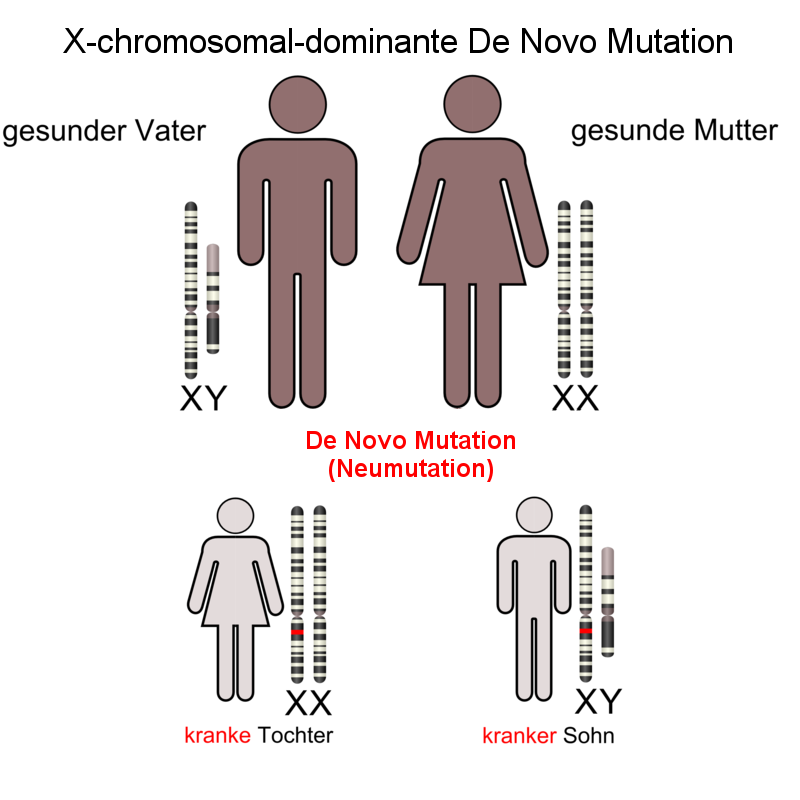
De novo mutations are so-called new mutations, i.e. neither parent is a carrier or affected themselves, instead the change occurs spontaneously. The mutation can reappear in the germ cells of the parents, sperm or egg, or in the early development of the fertilized egg in the womb. This is the case with almost all BPAN-Affected by the case:
BPAN is associated with a dominant new mutation in the gene WDR45 in the X chromosome. Here, too, dominant means that one defective gene is sufficient to cause the disease to break out.
However, since there are many more female than male patients with BPAN, it can be assumed that the additional X chromosome helps girls to compensate for the loss of function of the WDR45 gene somewhat better, while boys who only have one X chromosome are assumed to often not survive pregnancy.
There are also exceptions to BPAN: There are individual cases of male BPAN sufferers in whom the mutation is caused by X-linked recessive inheritance was transmitted by the mutation-carrying but healthy mother.
Sources:
Patient-centric Description of the disease from dem AXIS Network (German)
The karyogram is in the public domain and was taken from Wikipedia: https://de.wikipedia.org/wiki/Karyogramm#/media/File:DNA_human_male_chromosomes.gif
Figures on autosomal recessive and autosomal dominant inheritance: Kuebi = Armin Kübelbeck – own work, people taken from Image: Autorecessive.svg made by en:User:Cburnett, made with InkScape. PNG-File derived from SVG master, CC BY-SA 3.0, https://commons.wikimedia.org/wiki/File:Autodominant_01.png, https://commons.wikimedia.org/wiki/File:Autodominant_01.png#/media/File:Autorecessive_01.png
Figure of the X-linked dominant De Novo mutation: Noah Rusch, compiled with Gimp and supplemented by two illustrations (https://commons.wikimedia.org/w/index.php?curid=3755086#/media/File:X-chromosomal-dominant-Vater.png and https://commons.wikimedia.org/w/index.php?curid=3755086#/media/File:X-chromosomal-dominant-Mutter.png) by Kuebi = Armin Kübelbeck, CC BY-SA 3.0
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}